
First of all, the basis for this test is that dogs with pituitary-dependent hyperadrenocorticism (PDH) or functional, cortisol-secreting adrenal tumors (FAT), because of their increased adrenocortical mass or volume, have the capacity to secrete excessive amounts of cortisol.
This is an indirect test that gauges the degree of adrenocortical thickness. Unlike the low-dose dexamethasone suppression test, the ACTH stimulation test doesn’t look at the entire hypothalamic-pituitary-adrenal (HPA) axis or the effect of glucocorticoid-negative feedback on the HPA axis.
But what’s the percentage of dogs with Cushing’s disease that are actually diagnosed with this test? What’s the test sensitivity?
About half of dogs with cortisol-secreting adrenocortical tumors and about 80% of dogs with pituitary-dependent hyperadrenocorticism (PDH) show an exaggerated cortisol response to the ACTH stimulation test.
In clinical practice and reality, however, the sensitivity is actually worse than those statistics reveal. Although it is clear that over 20% of dogs with Cushing's syndrome have post-ACTH cortisol test results within the reference range (< 20 μg/dl for my laboratory), an additional 20-30% of dogs with Cushing's have test results described as "borderline" (serum cortisol concentrations >16 μg/dl but <24 μg/dl).
In effect, that means that only 50-60% of dogs with Cushing's disease will have serum cortisol responses that are clearly abnormal (> 25 μg/dl). In other word, this test is a poorly sensitive diagnostic test for Cushing’s syndrome. In most dogs, it would be more cost effective to turn to another test, such as the low-dose dexamethasone suppression test, as the first-line screening test.
Other disadvantages to using the ACTH stimulation test:
In addition to the ACTH stimulation test’s mediocre test sensitivity, there are 2 other reasons for choosing one of the other diagnostic tests over the ACTH stimulation test, including the following.
- First, of all, the cost of the preferred ACTH (cosyntropin; Cortrosyn) is high. I’ll discuss more about why you need to use cosyntropin in my next post (I’ll also offer my suggestions on how to extend the shelf-live of Cortrosyn to make it more cost effective).
- Secondly, this test cannot determine the underlying cause of Cushing's syndrome. In other words, a positive ACTH stimulation test doesn't tell you whether the dog has PDH or FAT, so additional testing will always be needed to determine that. It is a true screening test, and no features of the ACTH stimulation test result allow discrimination between PDH and FAT.
Yes, there are definitely 3 situations in which ACTH stimulation testing would be indicated as a diagnostic or monitoring test for adrenal disease in dogs. The major indications for using the ACTH stimulation include the following:
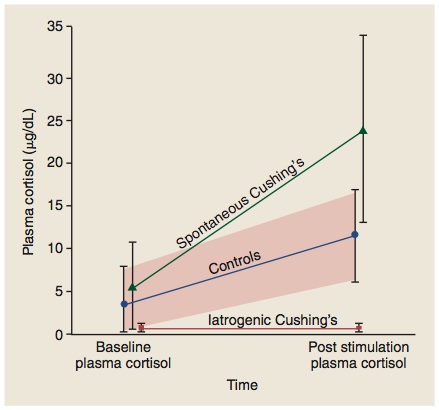
- Best test to diagnose iatrogenic hyperadrenocorticism in dogs. If the dog has clinical and laboratory features consistent with Cushing’s syndrome (e.g., polyuria, polydipsia, polyphagia, pot-belly, truncal hair loss, high serum alkaline phosphatase) but has a recent history of glucocorticoid use, this is the test of choice. If the cortisol response to ACTH stimulation is low-normal or blunted in this dog, the diagnosis would be iatrogenic Cushing’s, rather than the naturally occurring disease. None of the other pituitary-adrenal function tests can make this differentiation.
- Best test to use for monitoring and adjusting mitotane or trilostane therapy. Again, this is the only pituitary-adrenal function test that can be used in this situation; none of the other pituitary-adrenal function are useful in monitoring drug treatment.
- “Gold Standard” test to diagnose spontaneous hypoadrenocorticism (Addison’s disease). This is true whether the dog has primary or secondary hypoadrenocorticism or typical or atypical disease; the ACTH stimulation test is the only test to use for this diagnosis. As you can see in the figure below (an Ad from the company that manufactures Cortrosyn), the main indication for ACTH as a diagnostic test is adrenocortical insufficiency, not Cushing's syndrome.

In almost all cases, it is better to use stimulation tests to diagnose endocrine hypofunction, whereas suppression tests are best used for endocrine hyperfunction.
So with the ACTH stimulation, the 3 situations (listed above) where this test really has advantages over the other screening tests all include situations where the adrenal glands have been suppressed (iatrogenic steroid use, trilostane, mitotane) or destroyed (Addision’s disease)!
23 comments:
is there any benefit to using the combined LDDST-ACTH stim test?
The combined dexamethasone suppression test- ACTH stim test generally uses a HIGH dose of dexamethasone, not a low dose. I see no advantage in using that combined test, and do not recommend it.
Let's say you first do a classical 8-hour low-dose dexamethasone suppression test. Then at 8 hours, you inject Cortrosyn and do a 1-hour ACTH stimulation test, I don't have a problem doing that combination. But have you really gained that much? And it really becomes a long day!
Hello,
It is my understanding that when diagnosing a diabetic dog suspected of having HAC, the ACTH stim test is preferred because it is less sensitive and therefore less susceptible to false postives. Is this true? If so, can you please explain why and if not, then what is the best test to do under this circumstance especially if controlling the diabetes before hand is not an option? Thank you
You are correct that the ACTH stimulation test has the best test specificity of any of the 3 screening tests. In other words, you would be less likely to falsely diagnose a dog with Cushing's based on the results of an ACTH stimulation test than you would using the LDDST or UCCR tests.
That said, none of these screening tests for Cushing's are very good diagnostic tests when we are evaluating dogs with known nonadrenal disease. The "best" diagnostic test for Cushing's disease is and always will be a good history and physical examination.
Both dogs with Cushing's and diabetes will show signs of PU/PD, have hepatomegaly, and have high serum alkaline phosphatase activity. So we have to start looking at other signs, generally those of the skin or hair-coat, to really know if hyperadrenocorticism is also contributing to the signs seen in your dog with diabetes.
This can be a difficult diagnostic challenge (ie, making the correct diagnosis of concurrent Cushing's syndrome in a diabetic dog). But in my mind, it is almost always better to err on the side of not over-diagnosing Cushing's syndrome than it is to make a false diagnosis of the disease when it really isn't there!
Hello..our poodle is between 15/16 kg and it has been requested that he had 60mg of vetoryl .Yet I have read that the Dechra web site which suggests a lower dose .Please could you advise
Regards Peter
I generally start with a dose of 2 mg/kg per day, so I'd start with 30 mg per day in your dog. That said, some dogs will need a much higher dose.
What if a dog had the LDDST that came back negative but he has the classic symptoms for Cushing's? Is this a test that should be used then or is something else better?
Then an ACTH stimulation test or determination of urinary cortisol"creatine ratio should be used. In some dogs, repeating the LDDST in 1-3 months will be diagnostic.
We have a diagnostic conundrum which the ACTH stim may solve, but are confused about protocol. The case is a long term atopic dog (8 yo castrated male Maltese) treated every other day with oral prednisone for "years", now showing clinical signs of hyperadrenocorticism such as calcinosis cutis, pot belly, alopecia etc. Can we do the ACTH stim while the dog is using prednisone; we are worried the drug will measure as "cortisol" in the test leading to equivocal results. Or, do we withdraw prednisone over a week or so (risk of Addisonian crisis?) then test?
Very good question. First of all, what dose of prednisone (mg/kg body weight) is the dog getting on the alternate days? Most dogs do not develop iatrogenic Cushing's unless this dose is quite high.
In any case, the half life of pred is not that long in the bloodstream. I would go ahead and do the ACTH stimulation test on the day the dog does NOT get any prednisone (no drug for at least 24 hours). That should be long enough to get reliable endogenous cortisol measurement.
So, if both the pre- and post-cortisol values turn out to be low, that would certainly be consistent with iatrogenic hypoadrenocorticism (as well as signs of iatrogenic Cushing's).
If the post-ACTH stimulated cortisol is high, then the dog likely has spontaneous Cushing's syndrome. This would not be unexpected in a Maltese!
From Jenny
I have a 12 1/2 year old cairn terrier who has abnormal liver function tests and who my vet is convinced he has cushings based on clinical signs. He is becoming more lethargic. He has had several ACTH tests but have all come back negative. My vet now wants to use a low dose dexamethasone supression tests after discussion with the laboratory, would you suggest this? Would it be worth me considering referral to someone like yourself?
Yes, the low dose dexamethasone suppression test is the gold standard test for Cushing's.
If you aren't happy, talk to your vet about a referral to an internal medicine specialist.
I certainly wouldn't make any definitive diagnosis based on what you have told me. I'd continue to monitor and maybe repeat the tests in 3-6 months. Talk to your vet.
I certainly wouldn't make any definitive diagnosis based on what you have told me. I'd continue to monitor and maybe repeat the tests in 3-6 months. Talk to your vet.
Dear Dr. Peterson,
is there a time limitation/waiting period for performing an ACTH-stim test after a previously performed LDDS test (i.e. could the one dose of dexamethasone administered suppress the adrenal axis enough to cause a falsely low increase in cortisol on my stimulation)?
Thank you,
P. Mueller DVM
Theoretically, you are correct. The baseline cortisol certain could be suppressed but the post-ACTH stimulated cortisol shouldn't be affected.
I'd try to wait a week between a LDDST and ACTH stimulation test, if possible
Dear Dr. Peterson,
I did an ACTH stim (0-1 hours)followed by a LDDST (2-9 hours) the same day for a patient in sequence that is coming from 6 hours away. Would I have to interpret the results separately.
Thank you
Cyrus
You can't do an ACTH stimulation followed by a LDDST on the same day. The ACTH stim test are okay but the LDDST don't mean anything if they aren't suppressed. The ACTH may continue to stimulate some cortisol for along time.
I have an 11yo, MN, crossbreed who has had urinary incontinence for the last 8 months (dribbling urine when lying down and when excited). He has a caudally displaced bladder based on abdominal radiography but I was concerned that this was not the only problem given the late age of onset (no previous urinary tract signs but could it just have been exacerbated by age related muscle weakness?). Blood tests reveal persistent and marked elevations in ALP over the last six months and I was concerned about Cushings disease as a predisposing factor but the owner reports no increase in thirst. LDDST is consistent with pituitary dependent hyperadrenocortism and there is mild to moderate vaculolar hepatopathy on cytology of hepatic FNAs. However, ACTH stimulation testing suggested normal adrenal function. Since the owner reports no polydipsia (and they have measured 24-hour water intake) I am unsure whether this is a false positive LDDST result or a false negative ACTH stimulation test result. The adrenal glands are both top end of normal range on US measurement. What would be your interpretation?
Dogs with Cushing's can develop overflow urinary incontinence, but then they have severe polyuria. This doesn't seem to be the case here. I'd focus of the owner's complaint now and do followup testing for possible Cushing's in a few weeks/months.
I have this case of an 8 year old German Shepherd who is PU/PD with an ALP of 865, ALT of 214, and a cholesterol of 412. She has weight gain and some mild focal (tail) hypotrichosis, and has a low free T4 by ED too (0.4 ng/dL A.K.A. 5.1 pmol/L).
The PU/PD, high ALP, and high cholesterol had/has me considering Cushing's too (her specific gravity is consistently low too) so I performed a LDDST on her. Her results are the following:
Baseline= 4.8 ug/dL (133 nmol/L) (norm= 1.0 to 6.0)
4 h post= 2.2 ug/dL (61 nmol/L) (norm= less than 1.5)
8 h post= 1.1 ug/dL (30 nmol/L) (norm=less than 1.5)
With these equivocal results, I am wondering if I should consider an ACTH stim??
Thank you for your time!
-Gabe
Yes, I would do an ACTH stim test or measure a urinary cortisol:creatinine ratio, or both.
Thank you very much!
Post a Comment