
First of all, the basis for this test is that dogs with pituitary-dependent hyperadrenocorticism (PDH) or functional, cortisol-secreting adrenal tumors (FAT), because of their increased adrenocortical mass or volume, have the capacity to secrete excessive amounts of cortisol.
This is an indirect test that gauges the degree of adrenocortical thickness. Unlike the low-dose dexamethasone suppression test, the ACTH stimulation test doesn’t look at the entire hypothalamic-pituitary-adrenal (HPA) axis or the effect of glucocorticoid-negative feedback on the HPA axis.
But what’s the percentage of dogs with Cushing’s disease that are actually diagnosed with this test? What’s the test sensitivity?
About half of dogs with cortisol-secreting adrenocortical tumors and about 80% of dogs with pituitary-dependent hyperadrenocorticism (PDH) show an exaggerated cortisol response to the ACTH stimulation test.
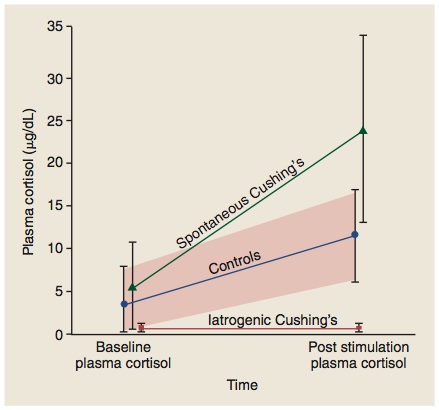
In clinical practice and reality, however, the sensitivity is actually worse than those statistics reveal. Although it is clear that over 20% of dogs with Cushing's syndrome have post-ACTH cortisol test results within the reference range (< 20 μg/dl for my laboratory), an additional 20-30% of dogs with Cushing's have test results described as "borderline" (serum cortisol concentrations >16 μg/dl but <24 μg/dl).
In effect, that means that only 50-60% of dogs with Cushing's disease will have serum cortisol responses that are clearly abnormal (> 25 μg/dl). In other word, this test is a poorly sensitive diagnostic test for Cushing’s syndrome. In most dogs, it would be more cost effective to turn to another test, such as the low-dose dexamethasone suppression test, as the first-line screening test.
Other disadvantages to using the ACTH stimulation test:
In addition to the ACTH stimulation test’s mediocre test sensitivity, there are 2 other reasons for choosing one of the other diagnostic tests over the ACTH stimulation test, including the following.
- First, of all, the cost of the preferred ACTH (cosyntropin; Cortrosyn) is high. I’ll discuss more about why you need to use cosyntropin in my next post (I’ll also offer my suggestions on how to extend the shelf-live of Cortrosyn to make it more cost effective).
- Secondly, this test cannot determine the underlying cause of Cushing's syndrome. In other words, a positive ACTH stimulation test doesn't tell you whether the dog has PDH or FAT, so additional testing will always be needed to determine that. It is a true screening test, and no features of the ACTH stimulation test result allow discrimination between PDH and FAT.
Yes, there are definitely 3 situations in which ACTH stimulation testing would be indicated as a diagnostic or monitoring test for adrenal disease in dogs. The major indications for using the ACTH stimulation include the following:
- Best test to diagnose iatrogenic hyperadrenocorticism in dogs. If the dog has clinical and laboratory features consistent with Cushing’s syndrome (e.g., polyuria, polydipsia, polyphagia, pot-belly, truncal hair loss, high serum alkaline phosphatase) but has a recent history of glucocorticoid use, this is the test of choice. If the cortisol response to ACTH stimulation is low-normal or blunted in this dog, the diagnosis would be iatrogenic Cushing’s, rather than the naturally occurring disease. None of the other pituitary-adrenal function tests can make this differentiation.
- Best test to use for monitoring and adjusting mitotane or trilostane therapy. Again, this is the only pituitary-adrenal function test that can be used in this situation; none of the other pituitary-adrenal function are useful in monitoring drug treatment.
- “Gold Standard” test to diagnose spontaneous hypoadrenocorticism (Addison’s disease). This is true whether the dog has primary or secondary hypoadrenocorticism or typical or atypical disease; the ACTH stimulation test is the only test to use for this diagnosis. As you can see in the figure below (an Ad from the company that manufactures Cortrosyn), the main indication for ACTH as a diagnostic test is adrenocortical insufficiency, not Cushing's syndrome.

In almost all cases, it is better to use stimulation tests to diagnose endocrine hypofunction, whereas suppression tests are best used for endocrine hyperfunction.
So with the ACTH stimulation, the 3 situations (listed above) where this test really has advantages over the other screening tests all include situations where the adrenal glands have been suppressed (iatrogenic steroid use, trilostane, mitotane) or destroyed (Addision’s disease)!










